We’re here to help.
Our friendly team is available to help Monday to Friday 9:00am – 5:00pm.
If you need urgent assistance, do not use this service. Call 111, or in an emergency call 999.
Our friendly team is available to help Monday to Friday 9:00am – 5:00pm.
If you need urgent assistance, do not use this service. Call 111, or in an emergency call 999.
0 items in your cart

Fast, discreet delivery
Free delivery over £40
100% UK-based pharmacy
All doctors & pharmacists UK-based
Free advice & support
Clinical support free · Mon–Fri 9am–5pm
Why Patients Choose Access Doctor
10+
Years serving UK patients
2,000+
Verified patient reviews
1,000+
Licensed treatments
24/7
Consultation available
Azithromycin tablets belong to a group of medicines called macrolide antibiotics. It is used to treat infections caused by certain bacteria including Chlamydia.
Order before 3pm — same-day dispatch (MON - FRI)
~5 min consultation
Secure & confidential · Reviewed by a UK prescriber
Azithromycin tablets belong to a group of medicines called macrolide antibiotics. It is used to treat infections caused by certain bacteria including Chlamydia.
Azithromycin is an antibiotic from a group called macrolides, and it has been used to treat chlamydia for decades. It works by binding to a particular part of the bacterial ribosome (the cell's protein-making machinery) and stopping the bacteria from producing the proteins they need to survive and multiply. Chlamydia is an unusual organism — it actually lives inside human cells rather than between them, hidden away in small membrane-bound compartments called inclusions. Azithromycin is particularly well suited to dealing with that, because it concentrates inside cells and tissues at far higher levels than in the bloodstream, and it has a very long half-life (around 68 hours), which means it lingers exactly where the bacteria are hiding for days after the last dose.
This is one of the most important things to understand before reading the rest of these FAQs, because it's the reason your prescriber may suggest doxycycline rather than azithromycin even if you came in expecting the latter. Three things drove the shift in UK guidance from the British Association for Sexual Health and HIV (BASHH) in 2018. First, head-to-head studies have shown that doxycycline cures chlamydia slightly more reliably than azithromycin — typically around 98 per cent for doxycycline against around 95 per cent for azithromycin. Second, doxycycline performs noticeably better than azithromycin for rectal chlamydia infections, which matter particularly in men who have sex with men but are increasingly recognised in women too. Third, and perhaps most importantly, azithromycin has been linked to driving antibiotic resistance in Mycoplasma genitalium, another sexually transmitted bacterium that often co-exists with chlamydia and is becoming harder to treat as resistance grows. For all these reasons, doxycycline 100 mg twice a day for seven days is now the standard first-line regimen for uncomplicated chlamydia in adults in the UK.
Despite the shift, azithromycin remains genuinely important in several situations. The most common is pregnancy — doxycycline can't be used in pregnancy because of effects on developing teeth and bones, and azithromycin is one of the safer alternatives. It's also used when someone has an allergy to tetracycline antibiotics (the family doxycycline belongs to), where doxycycline simply isn't tolerated, or where adherence to a seven-day twice-daily regimen is genuinely unrealistic and a shorter course is more likely to be completed. So if your prescriber has chosen azithromycin for you, there's almost always a specific reason — and the medicine still works, just with the small caveats covered above.
The current UK regimen is azithromycin 1 g taken on the first day, followed by 500 mg once daily on the next two days — a three-day course totalling 2 g. This has replaced the older single-dose 1 g regimen, because the longer course gives slightly better cure rates and is also more effective in reducing the risk of treatment failure when Mycoplasma genitalium is unknowingly present. The tablets are taken with water and can be taken with or without food. If you're prescribed azithromycin in tablet form alongside antacids or indigestion medicines, take the antacid at least two hours before or after the antibiotic, because antacids reduce azithromycin absorption.
Azithromycin starts working as soon as the first dose is absorbed, but full eradication of the chlamydia organism takes several days, partly because the medicine has to keep working its way into the cells where the bacteria are hiding, and partly because chlamydia has a slow growth cycle. Symptom improvement, where there are symptoms to begin with (most chlamydia infections cause no symptoms at all), typically begins within a few days. The course is considered complete and effective seven days after the first dose, which is why the no-sex window — covered below — uses that same seven-day mark.
This is one of the most important practical points and one of the easiest to get wrong. You should avoid all sex — including oral, vaginal, and anal sex, with or without a condom — for seven days after the first dose of azithromycin. This isn't because the medicine is dangerous to a partner; it's because the infection isn't fully cleared until the antibiotics have had time to work, and having sex during that window risks passing chlamydia on or, if your partner is also infected and being treated, getting reinfected. Both you and any current sexual partner should complete treatment and observe the seven-day no-sex period before resuming, even if you both started treatment on the same day.
Most people tolerate azithromycin well. The most commonly reported effects are gastrointestinal: nausea, mild abdominal discomfort, and diarrhoea, which usually settle within a few days. Some people notice a temporary change in taste, occasional headaches, or mild dizziness. Less commonly, people develop a rash. Two rarer effects are worth knowing about. The first is an effect on the heart's electrical rhythm — azithromycin can slightly prolong something called the QT interval, which in vulnerable patients (those with existing heart rhythm problems, low potassium or magnesium, or taking certain other medicines) can occasionally trigger arrhythmias. The second is liver irritation, which is rare but real and is the reason azithromycin is used cautiously in people with significant pre-existing liver disease. Severe diarrhoea, particularly with blood, fever, or significant abdominal pain, can occasionally indicate a different bowel infection (Clostridioides difficile) and warrants prompt medical advice.
Yes — and this part of treatment matters as much as taking the tablets themselves. Chlamydia is often silent: around 70 per cent of women and around 50 per cent of men have no symptoms at all, which means your partners may have it without knowing. UK guidance recommends that all sexual partners from the last six months are notified, tested, and treated. If your most recent sexual contact was more than six months ago, that partner should still be informed because chlamydia can persist undetected for a long time. The conversation can feel awkward, but sexual health clinics offer partner notification services — sometimes called "contact tracing" — where the clinic can inform your partners on your behalf, anonymously if you prefer. This service is free, confidential, and exists precisely because partner notification is genuinely difficult to do alone.
A test of cure — repeating the chlamydia test shortly after treatment to confirm the infection has cleared — isn't routinely recommended for uncomplicated chlamydia treated with azithromycin in non-pregnant adults, because cure rates are high and persistent infection is uncommon. However, a test of cure is recommended in pregnancy (usually three to four weeks after treatment), in rectal infections, and in anyone whose symptoms persist or recur. Separately from the test of cure, current UK guidance recommends a re-test for re-infection at three months for everyone treated for chlamydia, regardless of symptoms — because re-infection rates are high (around 10 to 30 per cent within twelve months in some studies), often from an untreated partner or a new partner. The three-month re-test isn't checking whether the antibiotic worked; it's checking whether you've caught chlamydia again.
Yes, in both cases. Azithromycin is one of the antibiotics specifically chosen for chlamydia in pregnancy in the UK, precisely because it has a long safety record in this setting and because the alternative (doxycycline) can't be used. Treating chlamydia in pregnancy matters: untreated infection is associated with preterm labour, premature rupture of membranes, low birth weight, and neonatal infections including conjunctivitis and pneumonia in the newborn. A test of cure three to four weeks after treatment is standard in pregnancy. Azithromycin is also compatible with breastfeeding — only small amounts pass into breast milk, and the levels are not considered harmful to the baby.
Azithromycin has fewer interactions than some older macrolide antibiotics, but a few are worth flagging. It can increase the effect of warfarin, raising the INR and the risk of bleeding, so anyone on warfarin will need extra INR monitoring during and after the course. It can raise levels of digoxin and certain statins, and it should be used cautiously alongside other medicines that can affect heart rhythm — including some antipsychotics, certain antimalarials, and a handful of other antibiotics — because of the QT-prolongation effect mentioned earlier. Antacids and indigestion medicines can reduce absorption if taken at the same time, so space them by at least two hours. As always, tell your prescriber about everything you're taking, including herbal remedies and over-the-counter products, so any interactions can be considered properly.
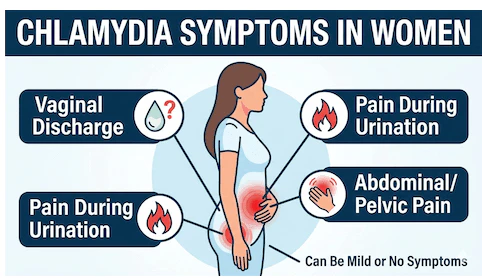
This is one of the most useful things to understand about chlamydia, because the absence of symptoms is one of the reasons it causes so much harm at population level. Untreated chlamydia in women can spread upwards from the cervix into the uterus and fallopian tubes, causing pelvic inflammatory disease (PID). PID is often silent itself, but it can scar the fallopian tubes and lead to long-term complications including chronic pelvic pain, ectopic pregnancy, and tubal-factor infertility. In men, untreated chlamydia can cause epididymo-orchitis (a painful inflammation of the testicle and adjacent structures) and, very rarely, fertility problems. Both sexes can develop reactive arthritis, a post-infectious joint inflammation. Treating chlamydia early — even when you feel completely well — is the single most reliable way of avoiding all of these outcomes, and it also helps protect future partners.
Persistent or recurrent symptoms after a properly completed course of azithromycin are uncommon but important. The first thing a clinician will consider is whether the original diagnosis was correct, or whether another infection — such as Mycoplasma genitalium, gonorrhoea, or trichomoniasis — has been missed or has co-existed with the chlamydia. The second consideration is re-infection from an untreated partner, which is the most common reason chlamydia "comes back". In rectal chlamydia, persistent infection is more common with azithromycin than with doxycycline, and a switch to doxycycline (or in some cases longer courses) may be needed. If symptoms haven't cleared by two to three weeks after finishing treatment, or if they return, a sexual health clinic or your prescriber can repeat testing and review the plan.
True azithromycin resistance in Chlamydia trachomatis itself remains uncommon, although there is some concern about a slight rise in treatment failures over the last decade. The bigger resistance issue, as touched on earlier, is in Mycoplasma genitalium — a related sexually transmitted bacterium that often co-occurs with chlamydia and that has become rapidly more resistant to azithromycin worldwide. This is one of the main reasons UK guidance has shifted to doxycycline as first-line treatment: not because azithromycin is failing for chlamydia outright, but because using less azithromycin protects its usefulness against M. genitalium and other infections where the alternatives are even more limited. From a patient point of view, the most useful contribution to slowing resistance is simple: complete the course you've been given, don't share antibiotics, and don't rely on partial or repeat courses without proper testing.
A few situations call for in-person assessment rather than treatment alone. A first-ever positive chlamydia result is a good moment to have a full sexual health screen, because chlamydia and other STIs frequently travel together — a positive chlamydia test should always prompt at least testing for gonorrhoea, syphilis, and HIV. Any pelvic pain, fever, abnormal bleeding, testicular pain, or systemic symptoms warrant urgent review, as these can suggest complications such as PID or epididymo-orchitis that need different treatment. Pregnancy, recurrent chlamydia, persistent symptoms despite treatment, and rectal infections are all situations where a sexual health clinic is better placed than a quick online prescription. NHS sexual health services are free, confidential, and used to seeing exactly the kind of questions covered above — there's no need to feel embarrassed, and a brief in-person review now can prevent much bigger problems later.
Yes, a prescription is required. Azithromycin is a prescription-only medicine (POM), so it cannot be bought over the counter. You can get it through Access Doctor by completing a short online consultation, which is then reviewed by a GPhC-registered prescriber. If the treatment is suitable and approved, a prescription is issued and your order is dispensed and dispatched discreetly from our UK pharmacy. You can start the consultation here: https://accessdoctor.co.uk/consultation/chlamydia/ - current pricing is shown as part of the ordering process.
No reviews yet. Be the first to write one.
Helpful articles and clinical guides related to this treatment category.
Free consultation
Online review by a UK prescriber
Next-day delivery
Order before 3pm where offered
Discreet packaging
Plain outer packaging